Pharmacy-driven and on-site water treatment pilots for reducing water pollution by pharmaceuticals

The strategies and action plans established in the first pillar, form the basis of this second pillar. To mitigate pharmaceutical pollution in the Northwest European region, we aim to develop two solutions.
1. Medicine use
We carry out three transnational pilots, aimed at promoting sustainable practices, such as greener prescriptions, appropriate drug delivery and disposal, and improved patient adherence.
2. Wastewater treatment
We develop a wastewater treatment solution through four pilots utilizing advanced techniques at high impact sites, like healthcare units and hospitals, to remove pharmaceuticals at their source.
Pilots will be conducted in pharmacy practices and decentralized healthcare settings.
Medicine use
Pilot 1: Benchmarking tool
About 90% of medicine residues in water come from medicines that leave the body after use, as well as medicines that patients throw away incorrectly. Benchmarking population-level prescription data can influence the prescribing behavior of general practitioners (GPs) and local pharmacists. This was evidenced by a small-scale Dutch pilot project, where a visual map was made. In this map, GPs and pharmacists could see their prescription behavior and compare this with others at a regional level (see North Netherlands Medicine Map, REACT-EU-SNN project).
The lessons learned from this Dutch pilot, will now be incorporated in a tool to assist community pharmacists, GPs, and policymakers across the Northwest European region. This tool helps them to better understand current prescribing behaviors. We also expect this will lead to fewer prescriptions of medicines that are more harmful to the environment. As such, this benchmarking tool will contribute to preventing medicines entering the water system.
To demonstrate and validate this benchmarking tool, we’ll conduct a 12-month pilot in the Netherlands, Belgium, Germany and Ireland. During this pilot, GPs and community pharmacists will be asked to use the developed tool.
Pilot 2: Pharmacist-led interventions
Interventions led by pharmacists have shown that community pharmacies and GPs are essential in optimizing drug use. However, these interventions often overlook environmental aspects. To address this, pharmacist-led interventions should also consider environmental impact.
Examples where environmental considerations were included in pharmacist-led interventions, are the EU HAPPY PATIENT project and the New Medicines Services in Belgium. Within the PREWAPHARM pilot, these interventions will be expanded and scaled across the Northwest European regions. There will be a clear focus on optimizing patient care and reducing environmental impact. For the PREWAPHARM pilot, the focus will be on the prescription and use of antibiotics and cardiovascular drugs.
Interventions within this pilot include:
- Staff training
- Prescribing and dispensing tools
- Improved collaboration between pharmacists and GPs.
We’ll use surveys to assess barriers and incentives to expand the intervention to other high priority ecotoxic medications.

Pilot 3: From hospital to home
Roughly 10% of patients are referred to hospitals for medical treatment. Many receive medicines that pose high environmental risks. Upon patients returning home, these medicines can enter the water system.
We will develop a toolkit aimed at reducing environmental impact when patients return home. This toolkit includes deprescribing medications, educating patients on proper disposal, post-discharge coaching by community pharmacists, and more.

Wastewater treatment
Although medicine-focused actions are well suited to reduce the amount of ecotoxic pharmaceuticals entering the water system, medication is an integral part of qualitative healthcare. This makes preventing medicines from entering the water system completely, impossible. Therefore, wastewater treatment is also part of the solution. The goal is to treat water containing specific medicines as close as possible to the source before it enters the water system. We consider three different levels of treatment:
- Removal at specific departments within healthcare institutes;
- Removal at specific healthcare institutes where higher concentrations of (specific) medicines are expected;
- Removal at specific municipal wastewater treatment plants and combined sewer overflows, currently not falling under the UWWTP directive (where no quaternary treatment step is required).

Pilot 1: At-source water purification systems
In hospitals and healthcare facilities, certain medicines can be traced back to specific departments. For some departments, preventive measures such as using alternative medicines or lower dosages may not be feasible for safety reasons. Therefore, more technical solutions are needed to reduce the input of medicines into the water system.
While some hospitals in the Northwest European region are already treating wastewater from specific departments, these treatment systems are still rare.
In this pilot we aim to:
- Demonstrate and assess the practical and technical feasibility of these systems;
- Optimize existing technologies;
- Prove the effectiveness of these systems in removing targeted medicines and their metabolites, and their residual ecotoxicity to aquatic organisms;
- Identify barriers and incentives for widespread implementation.
In this pilot, we’ll assess two systems which are currently in place in hospitals in The Netherlands.
Pilot 2: At-source water purification systems at institutional level
In this pilot, we will demonstrate and evaluate sustainable treatment solutions for wastewater from (entire) healthcare institutions, exploring synergies with water reuse and energy efficiency. The goal is to assess and optimize (novel) technologies and combine them into innovative treatment trains to remove medicines and reduce the environmental impact of healthcare on the water chain. The pilot will be held at two hospitals in Belgium and Luxembourg.
We aim to:
- Demonstrate the applicability and effectiveness of the technologies to remove medicine residues;
- Highlight the benefit and limitations of on-site purification systems;
- Explore water re-use possibilities within healthcare facilities and their surroundings;
- Provide insight for business case development;
- Offer guidance for scaling up in the Northwest European region.
Pilot 3: Local treatment facilities
In this pilot, we aim to find solutions for medicine removal at small scale wastewater treatment plants and combined sewer overflows.
For larger wastewater treatment plants (WWTPs), the Urban Waste Water Treatment Directive prescribes that they should be equipped with an advanced purification step, called quaternary treatment. However, in the Northwest European region, there are many small-scale wastewater treatment plants, where no quaternary treatment step is obligated. As such, these treatment plants could become future hotspots of medicine residue into urban surface water. Combined sewer overflows (CSOs) could also become hotspots. As during intense rainfall, untreated wastewater is released into surface water to prevent flooding at treatment plants and their surroundings.
Small scale WWTPs and CSOs are often remote and scattered. Therefore, solutions to reduce medicine emissions must be robust, low energy, user-friendly, and easy to implement and maintain.
During this pilot we:
- Evaluate the performance of existing systems;
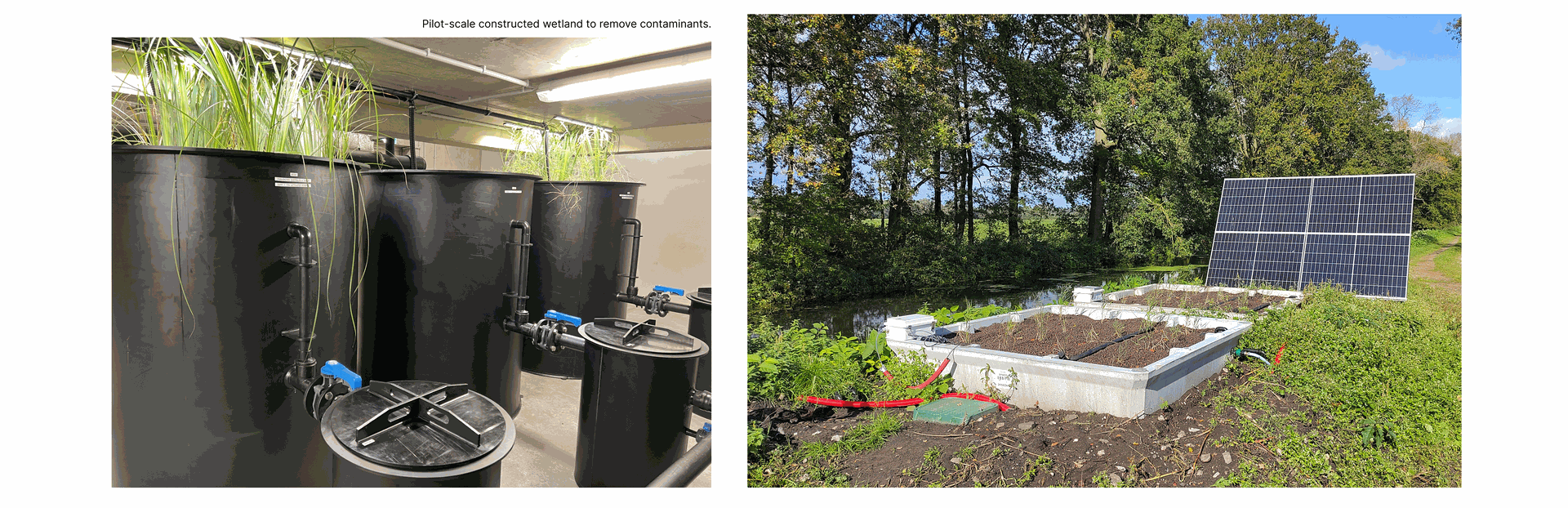
- Optimize and test suitable technologies at two test sites for removing pharmaceuticals, focusing on nature-based solutions in Belgium;
- Demonstrate the applicability and effectiveness of these technologies and highlight the benefits of additional treatment steps.
Pilot 4: Biological filter systems and development of bioaugmented filter systems
In this pilot, we aim to develop innovative microbial water treatment systems and combine them with existing technologies. Biodegradation is a safe, sustainable, and cost-effective way to remove medicines and their metabolites from water. Integrating biological treatment with conventional processes can enhance removal efficacy.
The success of biodegradation depends on finding the right micro-organisms. During this pilot we’ll establish a repository of microbes and microbial communities capable of degrading high priority pharmaceuticals as identified through the framework developed during the first pillar.
Microbes will be identified using high-throughput sequencing, and promising microbes will be enriched, isolated, sequenced, and evaluated in lab-scale bioreactors.
The findings, strategies and microbe repository from this pilot will be made publicly available for technology suppliers across the Northwest European region to enhance operational performance of their technology.
Contribution to joint strategy and action plans
Insights from each pilot (both medicine use and water treatment) will be compiled, outlining the benefits, challenges and key barriers and facilitators. This will provide input on the feasibility and potential for upscaling of the tested actions in the Northwest European region. At the same time, this will provide valuable insights for decision makers.
The pilot results will also inform impact assessment and scenario analysis. This includes using the findings to estimate outcomes throughout the Northwest European region. This will provide tangible, comparable data on the broader impact of implementing these solutions.
Communicating the results
We’ll share project results during our external events and via our website and LinkedIn. Matchmaking events will facilitate bringing our results to the stakeholders, learn from their suggestions and potentially include further questions in our pilot plans.
Make sure to follow us on LinkedIn and keep an eye on our website for updates. We are happy to hear your questions and suggestions! Reach out to us!

Prof. dr. Eelko Hak
Prof. dr. Eelko Hak is a professor of pharmacoepidemiology from the University of Groningen, he leads Pillar 1 & 2 and has been leading pharmacy-related environmental research since 2019.

Pieter-Jan de Buyck
Pieter-Jan De Buyck, R&D Project Lead at VITO, is responsible for Pillar 2 and has 10+ years’ water- sector experience developing solutions for industry and society.